Contraception/Chapter 6
By the Male.
Sheaths were first made of fine linen to encase the penis, and were originally called "preventives," as they appear to have been invented to lessen the liability to contract venereal disease. Sheaths are among the very earliest recorded preventives. See Gabriel Falloppio,[1] 1564, "De præseruatione à carie Gallica."
Monsignor Brown[2] stated also: "There is evidence that at the time of the Fire of London the condom was in use." They are still often advocated for the double purpose of prevention both of pregnancy and venereal contamination.
Present day "sheaths" are made in a great variety of thicknesses and quality, either of the cæcal membranes of animals or from various grades of prepared rubber. Their object is to collect the seminal fluid and prevent it coming in contact with the vagina. By the use of sheaths this object is generally achieved unless the condom breaks or is perforated. Owing to the fact that thinness of texture is very much desired (as even the thinnest condom interferes with the full sensory excitation) the very thin forms are in greater demand than those of stouter manufacture, and accidents or ruptures at the critical time are not infrequent.
Entirely similar in its physiological action in so far as it deprives the woman of contact with the glans is the short sheath, made to cover the glans penis only. It is less reliable and more difficult to adjust than the condom. The essential feature of the method, viz., the collection of the whole of the semen, is the same as the large sheath.
The sheath method in general, although a complete contraceptive if no rupture or perforation occurs, is very liable to unex pected insecurity through accident. The method has also a variety of physiological and psychological drawbacks.
In the first place it prevents contact between the glans penis and the vaginal tissues, and, therefore, robs the coital act of its full physiological benefit. It also robs the woman of contact with the seminal secretions (see p. 76) and thus is detrimental to her. It is also generally detrimental to the man in so far as it is to many unpleasant in use, and not infrequently with a man of not very strong sex capacity it reduces the potentiality for consistent erection and proper ejaculation. Many sensitive women find the odour of the rubber condom disgusting.
There are times, however, when the use of the condom appears almost imperative. In my opinion these are:—
- For the first week or two of marriage (see p. 183) in some circumstances.
- For men who are debilitated and suffer from premature ejaculation which is offensive to the bride.
- In cases of suspected venereal infection.
In this connection, however, we are departing from pure contraceptive requirements, and as I have often maintained contraception as such should be considered apart from the association of similar appliances in connection with the prevention of venereal disease. Nevertheless, owing to the ravaging prevalence of venereal disease the practitioner is often confronted with cases in which it is most valuable to be able to recommend procedure which will tend to operate both so as to prevent pregnancy and to reduce somewhat the risk of infection. (The condom, of course, does no more than reduce somewhat the risk of infection.)
In cases of uncontaminated persons, for other reasons its use is sometimes imperative. When it is a matter of life and death for the wife that no conception should take place, it is advisable for the man to use the condom in addition to any preventives used by the wife, because even with the greatest care there is always a slight risk of failure, in any one method, and when both parties take different methods of precaution the risk is reduced to a negligible minimum.
Much hindrance to progress in contraceptive knowledge has resulted from those advocates of control who ignore or deny the undoubted fact that there is truth in the contention of the clerical and "purity" schools of thought that "contraceptives are harmful"; for the condom is the contraceptive most generally known, and its recommendation by the medical profession has been weighty, and yet I maintain it does do much harm. Yet, as Hardy[3] says, "Professors Kraft-Ebing and Sarwey recommend its use in preference to all the other contraceptive methods. In 1905 at the Congress of Zürich organized by the Society to Combat Venereal Disease, the doctors were unanimous in favour of the sheath, indicating it as the only method to be recommended, both for the prevention of venereal disease and of conception." I dispute, however, the assertion of its entire harmlessness which follows. Dr. Robie, also, the American sexologist,[4] says "the condom is generally conceded to be the best arrangement" . . . . "as it allows of the complete satisfaction of the woman."
What may be described as the German school of sexologists favour it, and a typical quotation from their works is the following from Ivan Bloch's well known book,[5] "The ideal mechanical means (of prevention) is once more the condom. When it is used, coitus runs a perfectly normal course with the sole exception of the sensation during ejaculation." The coarse insensitiveness of attitude that can consider this last objection as existing, and yet state that the "act of coitus runs a perfectly normal course" seems to me deplorable. Yet this crude and ignorant statement has had a wide influence on men's attitude towards the whole subject. Bloch does not in this connection even perceive the great harm done to the woman by this method (see p. 127). Kisch also says that "When the man is fully potent the use of condoms can do no harm to the woman, since the only effect of the condom (in a very excitable woman) is to render the development of the orgasm a little more difficult, but not to prevent it." Kisch is emphatic in favour of the condom,[6] saying, "It is my opinion that the most trustworthy and least harmful measure at present available, and one preferable to all other mechanical apparatus, is a carefully selected and well made condom."
A remark, almost as crude, showing both ignorance concerning sensitive women's feelings and physiology is made by Freud,[7] who says, "Der Congressus reservatus mittels des Kondoms stellt für die Frau keine Schädlichkeit dar, wenn sie sehr rasch erregbar und der Mann sehr potent ist; in andern Falle steht diese Art des Präventivverkehres den anderen ein Schädlichkeit nicht nach."
Havelock Ellis (1921)[8] unfortunately follows these authorities, saying that "the condom is now regarded by nearly all authorities, as, when properly used, the safest, the most convenient, and the most harmless method."
Emphatically I dispute that the "authorities" are right.
It should be noted, of course, that Ellis's book, though dated 1921, takes no cognizance of books published since 1910 or so, and therefore he has not considered the arguments used in "Wise Parenthood," in 1918.
General Comments.—The condom for both emotional and physical reasons is not advisable for use in ordinary healthy coitus. It has its uses in connection with disease and danger, and for other special circumstances. In a general way it is inadvisable, as are, in short, all methods used by the male. On this point I lay great stress in spite of the fact that methods used by the male, and in particular the condom, are often recommended as offering more security than those used by the female. They are therefore of psychological value in cases of abject terror (see p. 186) but even in such they are not physiologically advisable.
This apparatus was brought to me by its inventor some years ago. It appeared to me wholly dangerous and absurd, but it may have got into use by some ignorant people. I know of no argument against its total condemnation.
Appliances used by the Female.
Specially prepared sponges in great variety are now on sale and in use, often made with a containing net so that they may be pulled out easily. There is, however, no necessity for these special sponges and in practical use it is far better not to have the attachment generally supplied with them, which increases the difficulty of keeping the sponge clean and disinfected.
The sponge has a particularly interesting place in the history of contraception in England, as it was the sponge "as used on the Continent" which was advocated in the "Diabolical Handbills" of 1823–4, and in the Republican in 1835 (see Chapter X on "Early History," p. 268).
There is much to be said for the sponge, and although some of the more modern practitioners greatly condemn it as being impossible to cleanse thoroughly, others still consider it the very best method for general use. Its principal advantages are that it is cheap, generally safe, very easy to manipulate, easily understood even by a stupid woman (and the stupid are exactly the people who most require birth control information, and who in the interests of the State should be encouraged to practise contraception). It does not require accurate adjustment as does the internal cap, and it can be used by the woman herself without the co-operation of her husband, which again is a point of racial value among the poor and illiterate, often overburdened, women whose husbands are either lascivious, careless or drunken.
The sponge used by itself without any chemical often succeeds, though on the whole it is an insecure preventive. Used in conjunction with a chemical powder, such as alum (see p. 114); quinine powder (see p. 104), or soap powder, or smeared with quinine ointment (see p. 105), soaked in vinegar and water or some other of the many possible spermaticides, the sponge is not only useful but is widely used and is recommended by some of the leading doctors as being the most satisfactory method.
In advising its use great stress should be laid on both the necessity and the difficulty of keeping it properly cleansed. Sponges of the modern rubber tissue have advantages over the natural sponge in being less inclined to harbour putrefying material. A patient should be advised not merely to wash out the sponge, but to keep it in a covered jar of some weak disinfectant such, for instance, as 1 in 20 aqueous boracic acid solution or ½ per cent. lysol.
The sponge is particularly useful for cases of abnormal cervices, either where the cervix is lacerated or proliferated when the application of an occlusive cap (see p. 189) is difficult or impossible. Also for cases where the cervix is depressed or has been removed. If the uterus is not prolapsed, then the sponge is safe and satisfactory for such cases.
In all cases of serious prolapse the sponge ´is useless, and in my opinion, the tradition of its unreliability has arisen from the fact that just the class of woman who tends to use the sponge (the poor and uneducated) tends also to suffer from neglected prolapse, which of course makes the sponge an unsuitable contraceptive, though they do not know that.
Comment.—The sponge is the most suitable contraceptive for various types of cervical abnormality. Nevertheless, in spite of this and of its particular value to poor and ignorant people who cannot afford or who cannot understand more precisely adapted contrivances, I do not greatly favour the sponge myself for general use and think that the internal cap (p. 138) is both more easy to keep clean and in many other ways more advantageous. The sponge, however, is preferable to any of the contraceptive means so far considered in these pages.
The general principle of these is similar to that of the sponge, the object being to fill up the whole end of the vaginal canal and with it to occlude the cervical entrance with or without some intercalated chemical. If cotton-wool or lint is used, it has the advantage of not requiring cleansing, as after use it is of course destroyed.
Here, perhaps, one may mention the various rather primitive methods of packing the end of the vagina, which are still used in the East, and are obviously of considerable antiquity. Such, for instance, as the very soft wads of silky native paper used in Japan. Under this heading also may be mentioned the balls and bundles of feathers used in India and elsewhere in Asia.[9]
Medicated tampons especially made to expand so as to fill the whole vaginal canal are, of course, widely used for other purposes. I do not know of any who have advised specially modified tampons for contraceptive use, but I myself have recommended the use of such tampons as contraceptives. The amount of expanding wool must, of course, be much less than in the usual tampon, as it should cover only the end of the vaginal canal, A specially prepared tampon may have very great medical advantages. I have myself advised a form which has been used with benefit containing ichthyol—ichthyol having, of course, definite curative properties well known to the medical profession. It appears also to act perfectly as a contraceptive. The use of a specially modified short tampon as a contraceptive is a method which many medical practitioners may find of specific use with their own patients.
Not only ichthyol, but a number of other preparations selected in accordance with the needs of the individual woman, could be administered in this way. The chief drawback to the method being the necessity of obtaining the specially prepared tampons, which are not cheap. The use of this method, therefore, would be confined to cases who are either really well-to-do, or who are patients sufficiently invalided to justify an expense much greater than is necessary for simple contraceptive means.
Comment.—I see in this method a suggestion, which is, in my opinion, most likely to lead to immediately useful advances in our knowledge of contraceptives. By the application of specially medicated tampons the combination of contraceptive means with locally curative applications might make great advances. Owing to expense, however, the method is not likely to come into general use, nor is it necessary that it should do so, as it is only suitable for cases of definite ailment and not for normally healthy women.
The general principle of all these dome-shaped pessaries, such as the occlusive pessaries and the varieties of the continental small "Mensinga," is the prevention of the spermatozoa from entering the internal os. This is achieved by the use of a small cap to fit over the cervical neck, thus putting a barrier between the spermatozoa and the egg-cell with the least possible interference or intervention of surfaces between the penis and vagina. The use of the small occlusive cap over the cervix leaves not only the greater part of the vaginal canal, but all the end of the vaginal canal round the cervical region in complete and natural contact with the male organ and with the seminal fluids. It interposes merely the barrier of thin rubber between the wandering spermatozoa and the entrance of the cervical canal. How necessary this is in many cases is shown by the occasional failure of both douches and antecedent quinine pessaries. Such failures sometimes appear to be due to individual carelessness, but at other times to that natural action of the fully excited uterus which must lead to inevitable failure for in the fully excited uterus the cervix may spontaneously open and interlock with the glans penis which thus discharges directly into the uterus, thus rendering inefficacious any quinine pessary or other chemical designed to lie in the vagina as a spermaticide. I have formerly hinted at this active co-operation of the cervix, but received critical comment, even denials of the possibility of the action. Such criticism is, however, due to the rarity of persons in whom this happens and the impossibility of demonstrating it, as it can only take place at the height of sex excitement. There is no doubt whatever, that some fully sexed and roused women do experience the interlocking of the glans penis with the cervical canal, and such a woman does aspirate some of the seminal ejaculate into the uterus.
It is of course arguable that it would be better that even the small area covered by the cervical cap should have no covering on the occasion of copulation, and to a certain extent I agree with this. Nevertheless if the type of cap which I advise is used then all the chief benefits of coitus are obtained and the interference with the complete normal sex act is at a minimum.
The form of cap which I advise, and the obvious advantages of which are confirmed by experience of a year and a half's use at the Birth Control Clinic[10] is given in diagrammatic form (p. 152, see Pl. iii, fig. 6). The centre or crown portion is of thin rubber, the rim being of either solid rubber or with an inflated air rim according to circumstances. Experience so confirms me in the view that the solid all-rubber rim is the best, that I advise no other, and at the Clinic we now always use the all-rubber solid rim. The essential point of the different features of the cap is that the crown should be large, high and thin, and of very perfect manufacture and the diameter should be measured across the inner side (as is the diameter of a hat) and not from the outside of the rim. The cap of this type, which has a great variety of modifications according to different makers, &c., is based on the small occlusive or Mensinga pessary, and the best variety, improved for use at our Clinic, goes under the name of the "Pro Race."
The whole cap is soft enough to be very easily pinched together for insertion, and when used, if the woman does not herself understand it, she should be instructed to insert it when sitting in the position of the Red Indians, namely, squatting on the heels. The cap should be pinched together with convex surface posteriorly and pushed up until it reaches the cervical canal and then allowed its natural expansion. As a rule it is found that it quite readily and automatically adjusts itself and only needs pressing into place round the cervical neck. All that is necessary has then been done. Some women, however, are stupid and nervous and may require to be shown and even to practise taking it in and out themselves during instruction. Experience at the Clinic with seventeen hundred poor and uneducated women has shown that ten minutes' instruction is quite sufficient under ordinary circumstances.
All the varieties of cap are usually sold with a ribbon or rubber attachment with which to pull it out. I find that this is inadvisable from several points of view. The most important objection to the woman tugging at the attachment is, in my opinion, the risk involved of drawing down or uncomfortably "sucking" the uterus. The properly adjusted cap adheres very tightly and mere pulling does not detach it, but it may induce elongation of the cervix or prolapse. Among opponents of contraception one of the whispered objections is that "methods cause prolapse"—and I fancy the grain of truth in this apparently ridiculous idea is due to the unintelligent tugging at the attachment of a well-placed cap. It is better for the attachments to be cut off, and when it is desired to remove the cap this should be done with a jerk of the finger under the rim which detaches it easily and with no risk of such injury. Caps can be obtained made without any attached loop, which is much the best. I should like to see only these advised until something even better is discovered.
When first instructing a woman the doctor should notice whether she has an abnormally long vaginal canal and unusually short fingers. If so, she will be unable herself to place the cap satisfactorily. In most women, however, the length of the vagina and the length of the first or middle finger are such as to make it quite easy for them to insert and remove the cap themselves.
Opponents of contraception have made much "copy" out of a case of a lady doctor who could not use the cap herself; from which the inference was drawn that the method was at fault! Whereas, in fact, the lady had particularly small hands and a long vagina, and it was merely a physical impossibility for her to reach her own cervical region. Such cases are rather infrequent, but as they attract much notice, each creates more impression than a hundred normal women.
The "Pro Race" and most other occlusive pessaries are made in three sizes, No. 1 or 2 being in general the size used by the average woman. Size No. 2 is found, after a good deal of experience, to be in much the greatest demand. If a woman has not suffered undue laceration at childbirth, even after she has had two or three children, size No. 3 is still too big for her and size No. 2 adequate.
In conjunction with the cap some prefer to use quinine ointment, smeared on it both internally and externally, partly to lubricate it in its passage up the vagina (which is often not necessary at all, or can be done more easily with slightly soapy water), and partly as an added precaution. This ointment, however, is not good for the cap.
It must not be forgotten that there is no foolproof method of birth control, except instruments kept under medical observation (see p. 173); and in critical cases it is advisable to use a combination of both the cap and a second method, preferably quinine, either in the form of ointment or of a quinine pessary. But with an intelligent, careful woman, properly fitted and instructed how to use the cap, the cap alone without any chemical is in most cases safe and sufficient, unless the woman is "incorrigibly fertile" (see p. 61). The reason for the safety of the cap is that it prevents the sperm entering the uterus (sperms, it should be remembered, may live even as long as seventeen days) and therefore confines the spermatozoa to the vagina where the naturally acid secretions of a normal woman should destroy their vitality.
One of the greatest advantages of the cap is a psychological one, namely, that it offers the very minimum of interference with the romantic side of the sex act. In this respect it is best used alone, because the quinine pessary may intrude on the consciousness, partly owing to its excessive greasiness and partly from the smell of the cocoa-butter, but the cap if used alone can be inserted some hours before bedtime, can be safely left undisturbed for twenty-four or forty-eight hours, and can be removed at any time next day for washing or exchange. Thus the woman can take the safeguarding precaution at the time of her ordinary toilet arrangements or while bathing, hours before it is required for use; hence there is no psychological interference with the coital act. The psychological and romantic value of this to all sensitive people is of the very greatest importance, as was mentioned in connection with douching (see p. 123). I know of a good many marriages which had been entirely jeopardized by the revolting necessity for the intrusive contraceptive procedure which had to be used until the pair heard of this unobtrusive cap method.
Some women, I am aware, have for many years used the cap quite regularly, leaving it in during the whole intermenstrual period; and abroad they are sometimes even advised to leave it in for two or three weeks undisturbed. Dr. Mensinga himself said of his pessaries: "Die Toleranz der Vagina gegen das Pessar ist sehr vershieden; im allgemeinen kann das Pessar, wenn gewünscht, beliebig lange Zeit, je nach Erfordern, sogar ruhig bis zur Eintrittazeit der Menses liegen bleiben." . . . "Einige weniger empfindliche Patientinnen lassen dasselbe sogar während der ganzen intermenstrualen Zeit unbehelligt liegen, andere nehmen es wöchentlich aus, auch zweimal wöchentlich, eine täglich. viele aber lassen es ruhig liegen, unter Gebrauch der Douche."[11] As unfortunately, in Britain nowadays, such perfect health as would would justify this advice is very rare, unless the medical practitioner is acquainted with the woman and sure of her exceptional health, it would be unwise to recommend this. It is probably always unwise to recommend this to working-class women. As a rule the woman should take it out every second day at latest, and leave it out for some hours at least for cleansing before re-insertion. It is better to have two caps in use, and employ an alternative cap each time.
The vaginal secretions of different women differ greatly in their destructive effects on the rubber of the caps. Some women can use the same cap almost uninterruptedly for a couple of years with almost no detrimental effect on the rubber; with other women the same standard make of cap will become distorted and unpleasant in a couple of months.
I think very much more has yet to be discovered about the chemical conditions of the vaginal canal and secretions; and that were contraception removed from its present neglected corner of medical study and considered openly and properly, true research on contraception and the vaginal reactions would lead to many discoveries of general value. There is little doubt that the degree of acidity of the vaginal secretions varies enormously in individual women, and it probably varies in the same woman under different circumstances (see also p. 61).
When a woman is using the cap the normal acidity of her vagina is probably a sufficient safeguard without any chemical pessary, because this acidity would destroy the motile activity of the sperm in a dozen hours or less. In any case, unless the woman is one of those who have a tendency to more permanent alkaline vaginal secretions, no other safeguard is necessary. In some women, however, motile sperm have been found many days after their deposition by the act of coitus. And in Taylor's work on medical jurisprudence[12] some very interesting cases, described by Bossi, art on record in which the spermatozoa lived in the vagina as long as seventeen days.[13] So far as I can discover no note was taken of the acidity or alkalinity of the vagina at the time, but I think in the case of extremely long vitality of the spermatozoa recorded, from what one knows of the general character of the spermatozoa, that in such exceptional cases for one reason or another (whether normal to her or not) the vaginal secretions in that woman must have been of the mildest acid, or more probably alkaline. In the ordinary way the modern woman's secretions are acid enough to dispose of the sperm in a few hours or at any rate by the next day, so that if she removes the cap when bathing the following day there is no need to use a douche of chemical solutions or any other substance.
In this connection I should like to comment on an interesting observation published by Kisch in quite another context, and without comment from him to link it on to the theory of contraception. Kisch said[14] (p. 216), "A special significance must be attached to the glands of the cervix uteri, which, according to my own observations, have the function of providing a secretion that increases the mobility of the spermatozoa, and this enables them more readily to find their way into the uterus. I have endeavoured, by a series of histological observations, to determine the properties of these glands and the changes they undergo in the different phases of sexual life. . . . These glands, which are lined with columnar. ciliated epithelium, are but slightly developed before puberty, being then simple excavations; . . . later, during the menacme, they become long dendriform, blind-ending glands, which during menstruation and under the influence of sexual excitement, furnish a secretion, variable in quantity, and in quality distinguished especially by its alkaline reaction." He then goes on to consider their pathological degeneration. Again on p. 300, after discussing details about conception Kisch says: "I further regard it as important in promoting conception, that simultaneously with the changes above described, the reflex nervous stimulation should lead to the secretion by the cervical glands of a gelatinous material, alkaline in reaction, and therefore adapted to increase the locomotive powers of the spermatozoa, so that these latter, aided by the activity of the ciliated epithelium lining the cervical canal, will gain the interior of the cavity of the uterus, and thence pass onwards to the Fallopian tubes."
These observations of Кisch appear to me to add very substantial arguments in favour of the use of the cervical cap as a contraceptive whenever security from conception is seriously desired.
Further practical details about the caps themselves may be useful. On the market are small rubber caps of many shapes and forms, generally with a solid rim, some with an air-inflated rim, others with spring rims, and all in a great variety of sizes and differences in the relations between the cap-like centres and the sides of the ring-like periphery. These originated from the continental "Mensinga," or small occlusive pessary, although the shapes now most in use are not exactly identical with the "original Mensinga" as figured by Mensinga himself. A great many registered or semi-trade names have been attached to variations of the small cap, the principle of which, whatever the variety, is essentially the covering over of the mouth of the cervical canal.
There is much to be said in favour of this general principle; indeed I think it is the soundest of all methods of contraception at present in use, but of the dozen or two modifications of the cap which I have seen, one only appears to me to be thoroughly reliable and satisfactory, the particular value of this depends on the relation of the size of the cap to the rim, &c. Caps with air inflated rims, and rims containing metal springs of various sorts, I do not like, and now I always give warnings against their use, both personally and through the clinic. The simple soft but firm rubber ring of the rim in the Pro Race is in every respect the best. Nevertheless, any of the dozen or two varieties of these things on the market may, in differing circumstances, suit individual cases. One of the main faults to be found in many brands is careless and hasty construction; the "seam for instance being joined so that minute perforations exist. The junction between the dome-like cap and the rim is often carelessly connected, or left very rough and difficult to keep clean. Also (an important point in the construction) the majority of the forms have what I consider too low a dome.
I have followed up various complaints of failure, or of inability to obtain exactly the article demanded, and have been surprised and disappointed at the variability of the cap which is sold as the small check or occlusive pessary. The relative sizes and proportions of the cap to its rim have a significance which it may be worth stating. In the accompanying diagrams A1 and A2 are drawings of
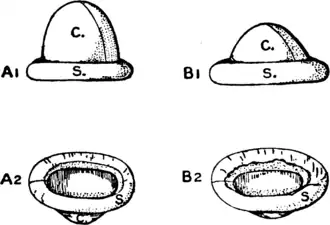
a satisfactory cap (see also Pl. 6, fig. iii), B1 and B2 are drawings of a type frequently sold, and in my opinion not only unsatisfactory on general principles, but liable to lead to those failures which have made some people distrust this most valuable method. The points to be noted in the drawings are primarily as follows: The Spring ring S and the conical portion C should be in such relative proportions towards each other as is indicated in A, and not as in B, where the rim is too thick and heavy and the conical portion C is too flat and small.
There are two interesting physiological reasons against too flat a cap, one depending on the characteristic of a good many women, namely, irregularity in the menstrual appearance, so that they may find themselves inadvertently wearing the cap at the commencement of the menstrual flow. A very small dome is then unsuitable; if the high domed type I recommend is used no anxiety need be felt, as it allows for the flow for several hours at least; a second reason for the high dome is found in some women of intense sex activity, in whom the orgasm gives rise to uterine secretions in some quantity, for which the large dome allows an exit. Furthermore with a large thin centre to the cap there is no risk of crushing the cervical canal, whereas the small hard central dome or the flat lens-shaped cap both tend to crush and interfere with the cervix. Moreover, the high thin central piece allows of invagination, if, as sometimes happens, the glans penis and the cervical os interlock at the time of passion (see p. 60). I know of no objection whatever to the high dome to counterbalance all these advantages, and can think of none.
The low dome may suit sexually inactive women with small cervical canals, but it does not suit the active pair, for the penis may attempt to invaginate it and, not being able to, may dislodge it instead. Hence I believe some cases of "failure of this method" are due to the use of the small domed variety by couples who should have had the high domed cap.
A further point to be noted in the construction of the cap is that the whole appliance, both rim and cap, should be or very pliable and soft rubber and should not be withered or wrinkled in the slightest degree. Also the line of junction indicated down the fine line in the drawings of C, should be entirely secure, and without the smallest thin area or perforation. I have had sent to me a cap, otherwise perfect, in which a minute bubble in the rubber just at this junction had developed into a hole more than large enough for the entry of the sperm. To ascertain that the line of
junction is secure, the cap should be held up to the light, stretched and examined, preferably with a magnifying glass. But it is far better in every way to use the Pro Race cap in which there is a seamless dome.
In figures A2 and B2 the caps are reversed and shown from underneath, and the line of junction between the soft cap C and the surrounding ring S is apparent. In A it will be noted that the junction is smooth and that the cap and ring merge into one another. But in B there is a comparatively rough welding of the thick raw edge of the cap C, which is—or may be—a very dangerous source of failure, as it is impossible to keep it really clean. No cap which is offered with such a rough interior should be accepted by a would-be purchaser.
It should be remembered that rubber tends to perish, even when not in use, and that to put away a cap dry for months or more, and then bring it into use may mean serious failure, owing to the development of small cracks. Rubber which is not in use is best kept under water, as it is in scientific laboratories. It is then discoloured, but its pliability is retained. A small china or celluloid pot or jar with a lid should be available, filled with water, under which the cap is submerged after it has been washed out and dipped into a simple noncorrosive disinfectant solution.
A cap very similar to the one I advocate for ordinary English women is specially prepared for Jewish women and used by Jewish midwives. It is of a very much larger size than anything we have found to be required by ordinary British women. This quite extraordinary difference in size raises an interesting question concerning the national characteristics of internal structure in women of different races. Here once again, proper study of contraceptive methods may bring to light features of general interest to all branches of medicine.
A very great variety of small occlusive caps are manufactured in many countries, and have been in use for over thirty years under a variety of special names. They have had the general approval of many medical men, and one variety, for instance, goes by the name of "Dr. Patterson's." The experience of many who visit the Clinic has now entirely confirmed the views I held tentatively some years ago, and I do not hesitate to advise strongly against all makes with "steel spring rims," air-inflated rims, and so on. At the Clinic experience has taught us to rely solely on the very best quality all rubber cap.
Comments.—Sir Francis Champneys, Bart., M.D., interrogated in cross-examination by the Birth Rate Commission: "The other method we have had commonly practised are fixed pessaries precluding the entrance of spermatozoa into the cervix?" And his answer to that was: "I have never known any physical harm result from them if they are kept clean."[15]
I have no hesitation in saying that the "Pro Race" type of cervical cap, if properly fitted and used correctly, is the best available method of contraception for normal and healthy women. (It is obviously unsuitable for prolapsed wombs and injured cervices, see p. 189.) A further advantage of this contraceptive measure is that the woman herself is responsible for its correct use, and she is safe even if her husband be drunken, careless, obstructive or antagonistic. The man has no discomfort from its use, for generally his penis cannot detect that it is there.
The addition of the sponge which is attached so as to cover the whole rubber cap (see Pl. iv, fig. 8) makes it possible to dip the cap into vinegar or a solution containing some other of the many spermaticides, and this double security is liked by some people. I think, however, that the method has all the disadvantages of the ordinary sponge, and destroys some of the great advantages of the rubber cap, namely, the ease with which it is cleansed, and also its lightness. I think continued use of a cervical cap rendered heavy by its attached sponge and the liquid it holds is more than likely to have injurious effects on some cervices. If the addition of the sponge is desired by any individual, I should prefer to advise a sponge of the ordinary kind separate from the rubber cap.
As is shown in the illustration (Pl. iv, fig. 7), this form of cap differs from the above in being a solid, heavy, lens-shaped, flat piece of rubber which is designed to close the end of the vaginal canal and not to fit specifically over the cervical canal. Curiously enough, although so much simpler in construction, it is much more expensive, and is therefore often foisted off on unsuspecting inquirers in the belief that, being more expensive, it is a "better article."
In my opinion it has a variety of quite serious drawbacks, and in a good many instances where there has been objection to contraceptive caps on the ground of harmfulness, the cap which was supposed to be representative of the occlusive cap was actually of this type. My main objections to it are that it crushes against the neck of the cervix, and thus tends to close or distort the cervix; that it allows no space for unexpected menstrual flow or for normal secretions exuded during coitus; and that being hard and firm it does not allow any possibility of interlocking between the glans penis and the cervical canal.
A complaint was made in writing to me of "failure" of my method. I asked to see the cap used, as I always do, and found it was the flat solid cap called "Dumas' Antigeniture." I pointed out this was not only not the type of cap I advise, but very fundamentally different from it; and was told by the woman that it must be better, as it is the same thing, only more expensive! Credulous patients should always be particularly warned against the common error that expensive remedies are better than simple good ones.
Comment.—I not only condemn this form of cap whatever its make, but regret that the objections which apply to it are often, through ignorance, supposed to apply to the true occlusive cap. This uncritical carelessness of those who condemn "caps" has done much harm.
This cap, as seen in the illustration (Pl. iii, fig. iv), differs from the other two in being a perfectly simple concave cap of thin rubber. It was described and figured long ago by Mensinga.[16] Essentially it is the segment of a sphere, approaching in size but not quite a hemisphere, and inserted in its edge without any very definite thickening, is a thin metal spring rim. In use this cap lies in the vagina convex side upwards, unlike the cervical cap, and is intended, not to cover the cervix in particular, but to close the whole end of the vagina. Some who use it profess great satisfaction with it, but there is a good deal of evidence that it is very unreliable and very difficult to secure absolutely in place in order to maintain its position. Fürbringer wrote against these caps many years ago, saying: "Their introduction requires as a rule a skilled hand," and "they easily get out of position," also "some of my patients have as a result of the constant manipulations acquired painful and persistent inflammations of the adnexa."[17] Though Fürbringer does not say so, it is clear that this is due to the large size of the cap and its stiff steel rim; the small, soft, all rubber cervical cap was not known to him when he advised the condom as being better than such caps as the above. The size used has to be so much larger than the natural size of the unstretched vaginal canal that the tendency is to expand the canal unduly, which is neither good for the man, nor good for the woman.
This cap is made in a very great range of sizes (in diameters from 40 mm. to 100 mm.) but sizes 65 mm. to 75 mm. are those most commonly used. This very fact substantiates the above objections to its use, because anything introduced into the vagina with a diameter of that size, even though placed diagonally in the vaginal canal, must essentially lead to an unwholesome stretching in the average woman. It is used widely in Holland, but from what I know of Dutch women they are somewhat different from the English in build. In this country it was taken up by Dr. Haire, and as he was actively advocating it I wrote the following letter to the Lancet,[18] which has not been answered:—
"In response to the challenge of Dr. Norman Haire to name the physiological objections I have to the Dutch cap he prefers to use, may I first welcome the fact that Dr. Haire has recently re-written the practical instructions issued by the Malthusian League, so that they now accept my main thesis, viz., that the best form of contraceptive is an internal rubber cap worn by the woman. The differences between the different varieties of cap are minor though not unimportant.
"My two main objections to the Dutch cap preferred by Dr. Haire are, put very briefly (1) It must be worn so as to cover the whole end of the vagina and depends on stretching the vaginal walls for its power to remain in position. For the same patient the diameter of the Dutch cap necessary is very much greater than that of the occlusive cap which does not stretch the vagina. The Dutch cap then stretches the vagina in such a way that certain movements of physiological value (particularly to the man), which ideally the woman should make, are then impossible. It is true that few women either know or practise complete physiological union in coitus, but that is no reason to justify the advocacy in general for normal women of an instrument which inherently prevents certain natural and valuable movements. The Dutch cap, however, is really useful for slightly abnormal cases, such as very fat women, those with injured cervices, &c. (2) My second objection is that it covers all the tissues at the end of the vagina and near the cervix, and these tissues are among the most sensitive (and probably absorptive) of the woman, and it is not good that they should be needlessly covered; they are not covered by the small occlusive cap.
"For these and other reasons I think the Dutch cap inferior to the small occlusive for normal women."
This I followed by further details in a new edition of "Wise Parenthood."[19]
This cap is still pressed upon the public by the Malthusian League regardless of the objections noted above, and of another and still more serious one: the metal band which forms the spring of the cap, as used by Malthusians, is not welded but is bound by rusting wire with rough cut ends. At our Clinic we had a few of these caps for use in special cases where the occlusive Pro Race cannot be used. There I soon noted rough projections under the rubber, which I cut open and found these raw wire ends under a very thin skin of rubber. If by chance they should be used by one of the types of women whose vaginal secretions are injurious to rubber, and she left it in too long—say a week or more—it obviously would be most likely that the thin skin of rubber over the rough wire would be broken, and the raw end of the common wire might well cause lacerations either in the vaginal surfaces or the glans penis of the husband. Here, it appears, may be that scrap of truth behind the mis-statement so often put into circulation by opponents of the movement for contraceptive knowledge, that "occlusive caps cause lacerations." The Pro Race occlusive cap (see p. 140) does not and cannot cause lacerations because it is an entirely soft, all-rubber article; yet this Dutch cap is sometimes mistakenly called an "occlusive," and as there may have been lacerations from the wires in it described above, we see now how "the cap method" may be condemned in general by either careless observers or definite opponents who attribute to one type of cap the faults inherent in another.
There is still a further objection to the "Dutch" cap, which soon revealed itself in those few used now and then at our Clinic; the circular outline of the cap, on which its safety is dependent, is often very transient. Caps only used two or three times as sample ones. for fitting purposes remained permanently out of shape in a few days—one of them, even after a single usage. Of course, if so large a cap is worn that the vagina is well stretched anyway, a slight distortion of the circumference of the cap would be of no moment; but I think a large cap which stretches the vagina has the serious disadvantages noted above; on the other hand, if a rather small cap of this type be worn so that the vagina is barely stretched enough to hold it in place, then the distortion of the circumference might well leave a gap between the cap and the vaginal wall at one region leading to failure, and such failures help to account for the idea that "caps are not safe."
Comment.—I condemn it for general use, and consider it unwholesome owing to the stretching of the vaginal canal, and the resultant evils.
If the caps are properly constructed the Dutch type would be useful in certain cases, as for instance for a woman with a very short forefinger, or a very fat woman with the local parts stretched and displaced, for in such it may be the only form of cap which she may succeed in placing correctly herself. On the whole, however, I am not particularly in favour of it, except as a "second choice" for special and difficult cases (see also p. 190).
The "Mizpah," when both parts are attached, looks very like the cap described above (number 22, p. 138), but it will be seen from the figure (Pl. III, fig. 5) that it has a double rim, the idea being that the thin cap portion which is detachable should be taken in and out and the solid ring left in place.
The general idea behind the use of the cap is similar to that discussed on p. 139, and need not be repeated.
As regards practical details this cap appears to me to have three major disadvantages. In the first place I do not see why a ring should be left in place when the whole cap can so easily be removed. There is no advantage and some possible harm from leaving a ring attached to the cervix. Owing to its double groove the ring cannot remain perfectly clean and therefore it ought to be removed. The second disadvantage is that in my opinion it is extremely difficult for most women to attach the soft portion of the cap to the ring when it is in place, and that being so, if the ring has to be removed in order to be attached to the soft portion of the cap there is no advantage in having the parts separate. The Mizpah is decidedly inconvenient in having the two portions detachable, and the single cap all in one piece is both easier to use, and much lighter, an important consideration.
Comment.—There are advocates of birth control, however, who favour this particular form of cap. In all these detailed matters individual women will be found who favour one or other variety of the cap because it suits their own particular needs.
The "Mizpah" has most of the general advantages of the occlusive cervical cap.
As it has a soft dome of sufficient size, it has not the disadvantages of No. 24, and may be recommended to those who like it on the understanding that they should not leave the ring so long in place as is generally advised.
This is a form of rubber cap somewhat allied to the Dutch cap (see PI. IV, fig. 9) but not circular. It is more limpet or turtlebacked in shape, and its zygomorphic form makes its insertion more difficult than that of the circular pessaries, as it is necessary for it to be correctly oriented and for the narrower end to be placed in the posterior and the larger end in the anterior regions of the vaginal sinus. Its placing is therefore rather difficult, and special forceps have been designed for its application. Its sole advantage appears to be that, once inserted correctly, it is very little liable to displacement.
It is used on the Continent for cases of abnormal cervix and other such difficult conditions, and is inserted by a medical practitioner or trained nurse.
I know of no single instance of its satisfactory use in England, and I should be interested to hear from any who-use it.
Balls (just the ordinary small plain rubber playing ball of soft rubber) were long since advised by Dr. Anton Nystroem.[20] The size used should be about 1⅛ to 1¾ inches in diameter. The principle of their application is similar to the Dutch cap (see p. 160) but they should avoid some of the disadvantages of those caps. They are, however, difficult to remove without discomfort. Some continental medical practitioners advise them.
I have never known any case of their use.
A variety of these large internal sheaths for the vagina are made in one form or another. For instance one is advertised as "Dr. Kings" another as the "Mother of a family." All have an oval inflated rim with a long condom-like sheath of thinner rubber attached. In theory they resemble the condom, being merely in one way a reversed condom applied as a lining for the vagina instead of a covering for the penis.
From the point of view of the woman they have all the disadvantages of the condom in so far as they prevent contact of the male organ and female epithelium, and hence also, of course, prevent the absorption of the seminal fluids. From the point of view of the man they have some of the same disadvantages as the condom, but they do avoid the personal discomfort to him which so often leads to a reduction of his erection after applying the condom himself.
Sometimes a woman is aware of her husband's contamination with venereal disease, and also his callous refusal to take trouble to prevent her infection. Such an unfortunate wife should certainly use this protective sheath; it is the only feminine method offering anything approaching safety from venereal infection. It may also be used with advantage if the gravity of an unexpected pregnancy is extreme, as it is a secure preventive.
It is curious that almost every amateur in contraception thinks first of a simple stud or button to plug the cervical canal. In the last few years I have had a large variety of these "inventions" brought to me. Also a great many varieties in current use are shown me from time to time by medical men and others. There seem no end to the shapes, forms and materials of such devices. From simple studs, not unlike a collar stud, to a complicated fluted metal instrument almost as large as a cigar, almost every range of variety and shape that could be imagined seems to have been fashioned by one person or another, and used successfully by women in some part of the world.
In general I think any simple stud or contrivance calculated merely to fill the lumen of the cervical canal, is theoretically unsound and probably detrimental in practice. Nevertheless, I know such simple studs are advised by some medical men, and used successfully, but in general I feel they are probably not very safe as contraceptives. For slightly "frigid" women they may be quite successful, but I cannot imagine them succeeding with a woman sufficiently strongly sexed for the natural opening and aspiration of the os during coitus. The smooth-stalked stud or button would simply drop out and be useless. The plugging of the cervical canal and consequent closing of the exit for any extruded secretion is also not to be recommended, and is a very different thing indeed from the covering over of the external os with a cap which allows sufficient space for the natural requirements of exuded secretions during coitus.
Nevertheless many distinguished Continental medical practitioners view these contrivances with not only approval, but with enthusiasm, and one learned M.D. from S. America with whom I discussed the matter at great length maintained his advocacy of a very simple stud-like form as the best contraceptive possible.
I do not propose to illustrate or go into very much detail about contrivances of this sort, which can be readily imagined.
An Austrian apparatus of silver called the "Uterop" may be mentioned here; it is designed to enter the womb itself and is supposed to be left in weeks at a time.
An extension of the same type of thing, called "Venor" is used in Germany, and is designed so as to fill the cavity of the uterus. Often I have heard foreign practitioners advocate such things but do not know of their use by practitioners of any standing in this country. It is evident that their use may be better than a fatal pregnancy, but that they cannot be advised for normally healthy women.
The "Gold Spring" or "Wishbone" pessary is a variety of "stud" or stem which has become rather well known from its use in the United States. It is so made as not to block the lumen of the os, and thus permits the exit of the natural secretions as they arise. It is a somewhat more carefully thought out variety of the "stud" form with a bifurcated stalk, long known and illustrated in this country, as, for instance, in Down Bros.' well known surgical catalogue in which are figured similar appliances which were invented and used thirty or forty years ago.
I am not aware who was the individual who first devised this particular form of pessary, nor who are the chief designers of the modifications. It is catalogued by Eissner, the makers in New York, as being "made after the design and suggestion of three prominent New York gynecologists." The "Gold Spring" is at present principally used in America, although it is also used to some extent on the Continent and in this country. I first discussed its use in certain circumstances in the sixth edition of "Wise Parenthood," because so far as I could discover it is the best available pessary which being once inserted by a doctor secures a contraceptive means which is out of the control of the patient. Therefore, at present, it should be valuable if properly used, because it might be applied to one of the greatest problems for those advocating a racially valuable practice of contraception, namely, to secure freedom from conception on the part of degenerate, semi-feeble-minded or carelessly drunken women who are incapable of giving the necessary thought or care to the use of contraceptives themselves, and who ought on no account from a racial point of view to bear further children.
When I drew attention to this method in this country I did so from first hand discussion with doctors practised in its wide and successful use in America, and I did so unaware that English doctors knew so little about it and that most had not the necessary technique either as regards its insertion or its after-care. This has now been revealed to me from a number of sources and I must therefore reserve my advocacy of it in this country until the English medical profession has more fully considered the conditions for its successful use, as it only leads to disappointment to describe results attained in another country to women who are tied to their native city. I have discussed it fully with a doctor who has had a thousand successful cases, and who pointed out that the size and proportion of the pessary should be made in accord with the individual woman using it (a point, I think, universally overlooked by practitioners in this country), and that it necessitates a continued supervision of the patient to the extent of an examination, removal and cleansing at intervals of two or three months, although I have also heard from others who use such an instrument that they inspect it in their patients only every six months.
Some of those who oppose contraception either on principle or from prejudice have attacked this method as an "abortifacient." This is essentially untrue and unfair; although carelessly inserted or neglected after its insertion it may become such, it must not be forgotten that anything improperly used—a crochet-hook or a finger may become an "abortifacient." A small illustration of the spring was given in the Lancet[21] with comments. Mr. Norman Haire, M.B., described the appliance as an abortifacient, but without first acquainting himself with the fact of its use by most responsible and important doctors in the United States and elsewhere as a pure contraceptive. Mr. Haire, M.B., again attacked the pessary, and also me for my "ignorance of medical matters" for advocating it. He is answered by the fact that simultaneously with the publication of his attack on me in the Lancet, the British Medical Journal published a letter from a medical practitioner not merely advocating its use, but its compulsory use! This doctor went farther than I should do at present, and said:[22] "In cases unable to maintain themselves or their children the woman should be temporarily sterilized by compulsion for varying periods—for example, by the insertion of the spring wish-bone pessary." On other points also I replied to Mr. Haire in the Lancet.[23] My knowledge of this type of spring is chiefly at first hand, from personal discussions, but recently I received a letter from an important American doctor who wrote: "You are quite right in believing that I have myself used it in suitable cases quite extensively for a number of years. It has proved in every instance quite effective."
When in America I met one of the New York Gynæcologists who himself was so confident of the method as a reliable contraceptive that he placed it first among all contraceptives and considered no other equal to it. I met also another medical practitioner who specialized in birth control and who had had a thousand satisfactory cases in which this spring had been used as a contraceptive. Altogether I know of over 1,056 cases of its successful use, as against one (and a doubtful second) of its failure, the latter due to neglect and improper use no impartial scientist could rest content to condemn a method on such data.
British divergence of medical opinion is due, I think, to the one or two recorded failures which have been given undue prominence by those who did not perceive the cause of the error in application of the method to an unsuitable patient.
It should be noted that there is a considerable range of sizes and variety of makes to suit the special configuration of the individual patient. A special carrier for insertion is required and after-care is essential. The medical practitioners who use it largely in America have special after-care nurses whose business it is to keep in touch with patients who have had the spring inserted.
Were such serious and proper consideration of the means of contraception devoted to the subject in this country as it deserves, the method might prove invaluable for use for the very type of person whom it is racially desirable that doctors should control and should not leave potent to conceive through negligence and carelessness. However, the pessary is now made either of silver, silver gilt, pure gold or platinum and is therefore too expensive for this class of patient. It costs about two guineas; hence until our country decides to spend money on prevention rather than expensive institutions to keep wastrels and the feebleminded, the cost takes it out of the reach of the very ones who most need a controlled contraceptive.
This method is, so far as I can' discover, the only one so far available which might be used to deal with cases which otherwise should be sterilized. Therefore, this method should receive consideration and study rather than uninformed condemnation.
One medical practitioner in New York told me that it was used in the first instance for women who did not conceive owing to the persistent closure of the cervical canal, the pessary was inserted in order to stretch the canal and keep it open. After being used for that purpose for a few months it was removed, pregnancy ensued and then after the desired birth it was reinserted with a view to keeping the woman free from further conception till such was again desired. It would take too much space to discuss the matter fully, but it should be borne in mind that the theoretical considerations guiding its use depend on the very important though too generally overlooked, distinction between fertilization and conception. The ovum may (though not likely) be fertilized, but the action of the spring is to cause the uterus to throw it off before conception takes place and while it is yet free-moving. In this connection the reader is advised to study the admirable chapters in Ballantyne's great work.[24]
The method in my opinion is not suitable for women who wish merely to space desired children, as it is said that if the "wishbone" is persistently used it tends to make the uterus disinclined to settle down with a true conception.
It has of course an advantage over all other methods in not requiring daily care, and therefore it interferes least with the psychological reactions of coitus, because once inserted it requires no further thought on the part of the patient beyond intermittent visits to her doctor to have it attended to, and can be forgotten by her for weeks at a time.
Case No. 2024. Woman with two children, the younger 9 months old and delicate. This case is interesting as she is the only one known to me who found the small occlusive cap pessary gave a sense of irritation although it was not uncomfortable. This patient urgently required a reliable method as she preferred death to having another child, her baby was extremely delicate and her husband in financial difficulties. The gold spring pessary was inserted by her family practitioner. Slight coloured discharge ensued for a couple of weeks and heavy menstrual periods for two months. A year and a half later she writes "up to now it has proved a tremendous success. I have had no discomfort after the first two months." As she was leaving England the spring was removed, and she writes "I shall certainly have it replaced. . . it has been my best friend."
Comment: I hesitate to advocate any varieties of the above methods for general use in this country at present, but there is no doubt that some modification or other of these appliances which penetrate the os have proved valuable in many cases and deserve attention. I feel that a doctor who takes the trouble thoroughly to acquaint himself with varieties of the method may be doing most useful service, particularly in connection with women physically incompetent again to be mothers and who yet either dread or are unable to afford the operation of sterilization.
In conclusion I may say that where the woman is healthy, with normal cervix and the usual relation between the length of the finger and the vaginal canal, without any hesitation I should always recommend the simple cervical cap of the "Pro Race" all-rubber type rather than any other contraceptive. Intelligent women by the hundred thousand have used such caps for forty years, and found them almost ideal. With this cap, according to circumstances, the woman can use additional soluble quinine pessaries without any great inconvenience to the spontaneity of the coital act.
In all ordinary circumstances between a normal pair I favour the use of the contraceptive by the woman rather than by the man, because there is no means of contraception used by the man which is not detrimental. By the woman, however, control of conception need involve no such detrimental effect, and she may use the sponge, the soluble quinine pessary, or, best of all, the cap with a minimum of interference with the reactions of complete coitus and a maximum of comfort and security. One or other, or all three, of these methods can be applied with the greatest of ease.
There are certain special cases which require rather different procedure which will be indicated in the next chapter.
- ↑ Gabriel Falloppio (1564): "De Morbo Galllico: Liber Absolutissimus." First ed. Pp. 65. Patavia, 1564.
- ↑ Report of the National Birth Rate Commission. Second ed. London, 1917. Pp. 184.
- ↑ G. Hardy: "How to Prevent Pregnancy." Paris, English edition. Pp. 95. See p. 45.
- ↑ W. F. Robie (1918): "Rational Sex Ethics." Pp. 356. Boston, 1918. See p. 214.
- ↑ Ivan Bloch (1909): "The Sexual Life of our Time in relation to Modern Civilization." Trans. from Sixth German edition. Pp. x, 790. London, 1909.
- ↑ B. H. Kisch (undated): "The Sexual Life of Woman." Engl. trans. by Paul. Heinemann, London. Pp. 686. See p. 408.
- ↑ S. Freud (1911): "Sammlung kleiner Schriften zur Neurosenlehre aus den Jahren, 1893-1906." Pp. 229. Leipzig, 1911.
- ↑ Havelock Ellis (1921) (1910): "Sex in relation to Society." Pp. xvi, 696. Philadelphia, 1921. See p. 599.
- ↑ See, for instance, reference in Felix A. Theilhaber (1913): "Das Sterile Berlin." Pp. 165. Berlin, 1913.
- ↑ The Mothers' Clinic, at 61, Marlborough Road, Holloway, N. 19. The first British Birth Control Clinic, founded in 1921. (See also p. 384.)
- ↑ Mensinga, Dr. Med (1888): "Facultative Sterilität." Part II, supplement. Pp. 80. 2 pls. Leipzig, Seventh edition. 1900.
- ↑ Taylor (edited by F. J. Smith), 1920: "Taylor's Principles and Practice of Medical Jurisprudence." Seventh edition, vol. ii. Pp. viii, 952. London, 1920.
- ↑ Bossi (1891): Gazzetta degli Ospitali, April 8, 1891. (Quoted from Taylor, as I regret I have not been able to see this journal.)
- ↑ R. H. Kisch, M.D. (no date): "The Sexual Life of Woman," English translation by Paul. Pp. 686, 97 illustrations. Heinemann, London.
- ↑ Report of the National Birth Rate Commission. 1917. "The Declining Birth Rate." Pp. xiv, 450. See p. 254.
- ↑ Mensinga (1888): "Facultative Sterilität," Part 2, supplement. Pp. 80, 2 plates. Leipzig, Seventh ed., 1900.
- ↑ P. Fürbringer, Dr. Med. (1904) in "Health and Disease in Relation to Marriage and the Married State," edited by Senator and Kaminer. See art., "Sexual Hygiene in Married Life," pp. 209-242. English translation. London and New York, 1904.
- ↑ The Lancet, 1922, vol. 203, No. 516, Sept. 9, p. 588.
- ↑ Marie C. Stopes (1922): "Wise Parenthood." Ninth edition. Pp. xii, 66. London, 1922.
- ↑ See p. 79 in G. Hardy's "How to Prevent Pregnancy." Pp. 94, 39 illustrations. Paris, 1916.
- ↑ Lancet, November 12, 1921, p. 1003.
- ↑ R. H. Vercoe (1922), letter in Brit. Med. Journ., No. 3216, August 19, 1922, p. 327.
- ↑ M. C. Stopes (1922), letter in Lancet, No. 5166, September 2, 1922, p. 539.
- ↑ J. W. Ballantyne, M.D. (1904), "Manual of Antenatal Pathology and Hygiene: the Embryo." Pp. xix, 697. 95 illustrations. Edinburgh, 1904.